Barr et al's well-intentioned paper is starting to lead to some seriously weird behavior in psycholinguistics! As a reviewer, I'm seeing submissions where people take the following approach:
1. Try to fit a "maximal" linear mixed model. If you get a convergence failure (this happens a lot since we routinely run low power studies!), move to step 2.
[Aside:
By the way, the word maximal is ambiguous here, because you can have a "maximal" model with no correlation parameters estimated, or have one with correlations estimated. For a 2x2 design, the difference would look like:
correlations estimated: (1+factor1+factor2+interaction|subject) etc.
no correlations estimated: (factor1+factor2+interaction || subject) etc.
Both options can be considered maximal.]
2. Fit a repeated measures ANOVA. This means that you average over items to get F1 scores in the by-subject ANOVA. But this is cheating and amounts to p-value hacking. This effectively changes the between items variance to 0 because we aggregated over items for each subject in each condition. That is the whole reason why linear mixed models are so important; we can take both between item and between subject variance into account simultaneously. People mistakenly think that the linear mixed model and rmANOVA are exactly identical. If your experiment design calls for crossed varying intercepts and varying slopes (and it always does in psycholinguistics), an rmANOVA is not identical to the LMM, for the reason I give above. In the old days we used to compute minF. In 2014, I mean, 2015, it makes no sense to do that if you have a tool like lmer.
As always, I'm happy to get comments on this.
Friday, January 02, 2015
Sunday, November 30, 2014
Misunderstanding p-values
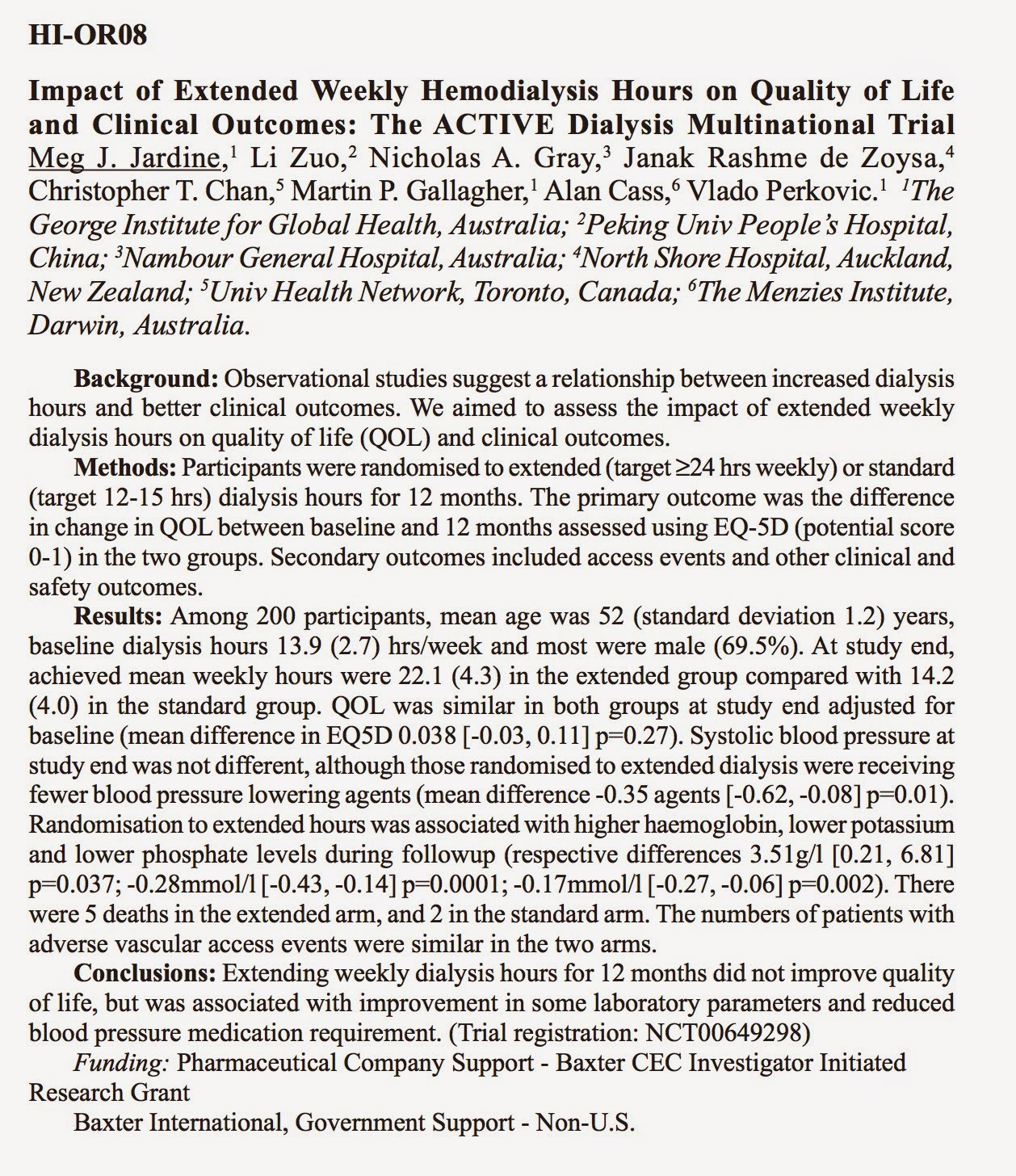
These researchers did a small between-patient study with low power to compare people on 24 hours of dialysis vs 12 hours of dialysis a week. They found that patients in the 24 hour arm had improved blood pressure (reduced intake of BP meds in the 24 hour arm), improved potassium and phosphate levels, and found no significant differences in a quality of life questionnaire given to the two arms. From this, the main conclusion they present is that (italics mine) "extending weekly dialysis hours for 12 months did not improve quality of life, but was associated with improvement of some laboratory parameters and reduced blood pressure requirement."
If medical researchers can't even figure out what they can conclude from a null result from a low powered study, they should not be allowed to do such studies. I also looked at the quality of life questionnaire they used. This questionnaire doesn't even begin to address important indicators of the quality of life of a patient on hemodialysis. A lot depends on the type of life the patient on dialysis was leading before he/she got into the study; what he/she does for a living (if anything), what other health problems he/she has,... These are the things that the questionnaire would measure; the questionnaire doesn't even tackle relevant quality of life variables associated with increased dialysis.
So, not only did they draw the wrong conclusion from their null result, the instrument they are using is not even the appropriate one. It would still have been just fine if they had not written "extending weekly dialysis hours for 12 months did not improve quality of life."
What a waste of money and time this is. It is really disappointing that such poor research passes the rigorous peer review of the Journal of the American Society of Nephrology. Here is what they say in their abstracts book:
"Abstract submissions were rigorously reviewed and graded by multiple experts."
What the journal needs is statisticians reading and vetting these abstracts.
If medical researchers can't even figure out what they can conclude from a null result from a low powered study, they should not be allowed to do such studies. I also looked at the quality of life questionnaire they used. This questionnaire doesn't even begin to address important indicators of the quality of life of a patient on hemodialysis. A lot depends on the type of life the patient on dialysis was leading before he/she got into the study; what he/she does for a living (if anything), what other health problems he/she has,... These are the things that the questionnaire would measure; the questionnaire doesn't even tackle relevant quality of life variables associated with increased dialysis.
So, not only did they draw the wrong conclusion from their null result, the instrument they are using is not even the appropriate one. It would still have been just fine if they had not written "extending weekly dialysis hours for 12 months did not improve quality of life."
What a waste of money and time this is. It is really disappointing that such poor research passes the rigorous peer review of the Journal of the American Society of Nephrology. Here is what they say in their abstracts book:
"Abstract submissions were rigorously reviewed and graded by multiple experts."
What the journal needs is statisticians reading and vetting these abstracts.
Subscribe to:
Posts (Atom)